
scoliosis
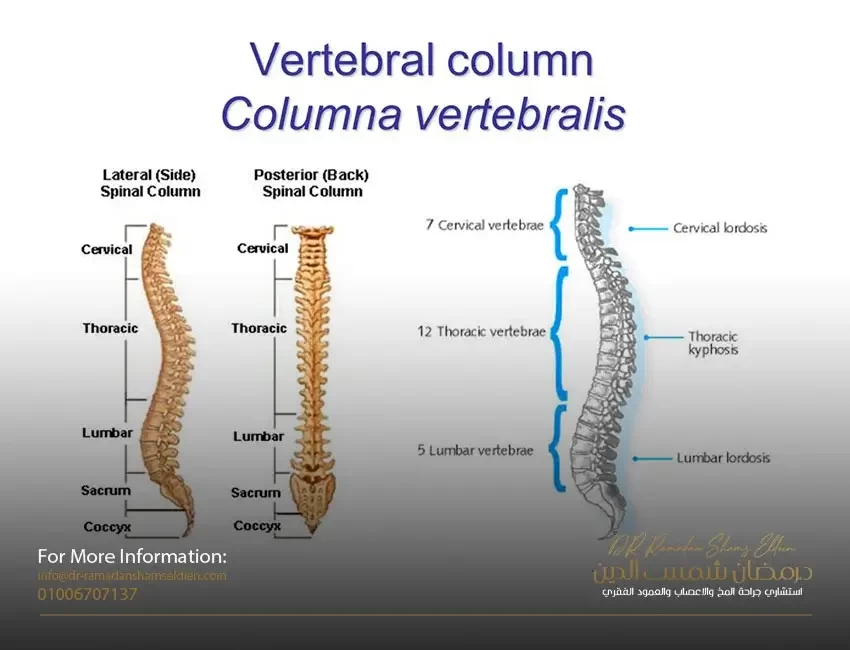
Scoliosis is a three-dimensional deformity of the spine and rib cage. It may develop as a single primary curve (looks like the letter C) or as two curves (a primary curve with a compensating secondary curve forming an S shape). Scoliosis may occur only in the upper back (thoracic) or lower back (lumbar), but it most commonly develops in the area between the thoracic and lumbar (the thoracic and lumbar areas). The doctor attempts to identify scoliosis by the shape, location, direction and size of the curve and, if possible, the cause. The severity of scoliosis is determined by the extent of the curvature of the spine and the angle of rotation of the trunk.
Determining and classifying the type of scoliosis often by the shape of the curve, by its location, or by its direction:
Scoliosis is classified according to the shape of the curve into structural (in other words true organic) or non-structural (which is functional or secondary). • In structural scoliosis, not only do the spine bend from side to side, but the vertebrae also rotate, resulting in a twisting of the spine . During torsion, one side of the rib cage is pushed out so that the spaces between the ribs widen and the shoulder blade protrudes (which causes the rib cage to deform or protrude); The other half of the rib cage is twisted inward, putting pressure on the ribs. • The non-structural or functional curve does not twist, but is a simple curve from side to side, and it is usually a compensation for the main structural curve or due to muscle spasms or other diseases of the vertebrae.
Determine scoliosis by its location. The location of the skeletal curve is determined by the location of the apical vertebra, which is the protruding vertebra at the apex (the highest point) of the spinal tuberosity. This particular paragraph will also undergo severe rotation.
Definition of scoliosis according to its direction. The direction of the curve in structural scoliosis is determined by whether the convex (rounded) side of the curve curves to the right or left. For example, a doctor defines a specific condition as right thoracic scoliosis if the apical vertebra is in the thoracic region (upper back) of the spine and the curvature is to the right.
The size of the curve is determined by taking length and angle measurements of the curve in an X-ray view.
Causes of scoliosis
First: idiopathic scoliosis
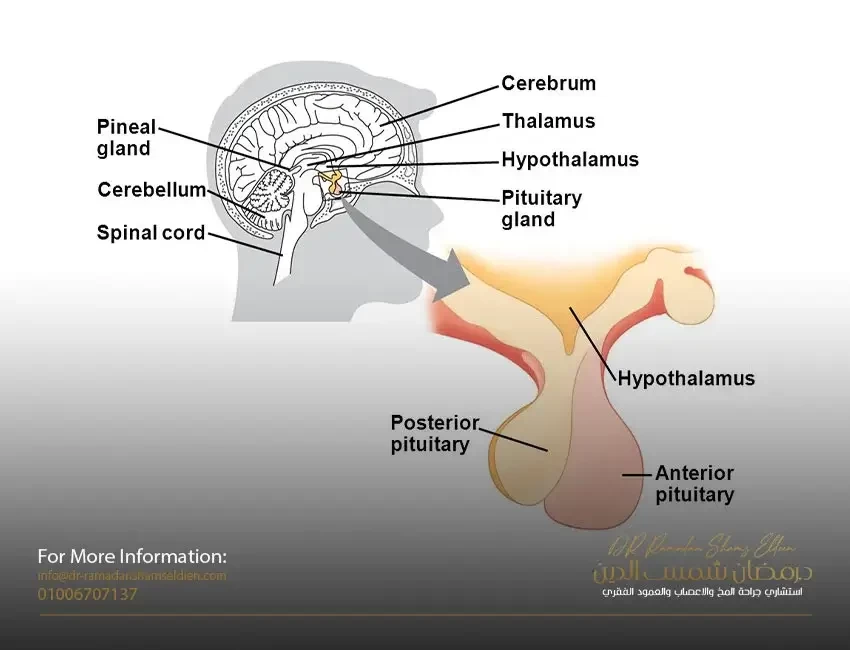
In 80% of patients, the cause of scoliosis is unknown. These conditions are called idiopathic scoliosis. Most cases of idiopathic scoliosis have a genetic basis, but researchers have not yet identified the gene or genes responsible for it. Researchers are investigating potential physical abnormalities that may cause bone or muscle imbalances that can lead to scoliosis. Among them are the following: muscles around the vertebrae. Some research suggests that imbalances in the muscles around the vertebrae may make children susceptible to spinal deformities as they grow. High arches in the feet. One study showed a higher incidence of abnormally high arches in the feet of people with idiopathic scoliosis, suggesting that altered balance may be a factor in some cases. Coordination problems. Some experts are looking at inherited impairments in cognition or coordination that may cause asymmetric spine development in some children with scoliosis. The investigators are also looking at possible abnormalities in collagen, an important structural protein found in muscle and bone. Other researchers are looking at a possible defective gene responsible for the production of fibrillin, an important component of the connective tissue that makes up bone and muscle. Some research has revealed abnormalities in a calcium-binding protein, calcodulin, among patients with scoliosis compared to the general population. Other researchers are still studying melatonin, a hormone secreted in the brain involved in sleep and growth. Animal studies and some human studies have found abnormalities associated with scoliosis.
Second: congenital scoliosis
Congenital scoliosis is caused by congenital abnormalities of the spine that usually involve abnormalities in the development of the vertebrae (missing or fused vertebrae). The condition usually appears around the age of two or between the ages of 8 and 13 as the spine begins to grow more rapidly, putting more stress on congenital malformations. Curves in such cases should be closely monitored, as they can progress rapidly. (Kidney problems, especially with only one kidney, often coincide with congenital scoliosis.)
Third: Scoliosis caused by genetic and medical disorders
Scoliosis may also be the result of muscle paralysis or deterioration from conditions such as myasthenia gravis, polio, or cerebral palsy. Other diseases that can cause scoliosis are Marfan syndrome, Friedreich's ataxia, Albers-Schönberg disease, rheumatoid arthritis, and osteogenesis imperfecta. Spinal cord injury may also cause scoliosis. A very rare genetic disease called familial dysautonomia has been identified as a cause of scoliosis in Jewish children of Ashkenazi descent. (It should be noted that only 500 cases have been reported globally, and this is related to the nature of the family composition of the Jews). Birth defects known to cause scoliosis include spina bifida or myelomeningocele (congenital hernia of the central nervous system).
Fourth: tumors of the vertebral column
Tumors and small growths or abnormalities in the spine may play a larger role than previously thought in the causes of scoliosis in young children. Back surgery to remove benign tumors increases the risk of spinal deformity.
Fifth: Causes of scoliosis other than structural or functional
Nonstructural scoliosis is sometimes caused by poor posture, leg length differences, and muscle spasms.
Scoliosis risk factors
General risk factors for idiopathic scoliosis. Idiopathic scoliosis (where the cause is unknown) is the most common form. It almost always occurs during a growth spurt just before and during adolescence. However, it can also occur in young children and even in infants. About 2% to 3% suffer from
Adolescents have a curvature of 10 degrees or more, but only about 0.3% to 0.5% have curves greater than 20 degrees. Mild curvature occurs equally in girls and boys, but curvature is 10 times more likely to occur in girls.
Medical risk factors. People with certain medical conditions that affect joints and muscles are more likely to develop scoliosis. About 10% of girls with Turner syndrome, a genetic disease common in women, develop scoliosis.
Young athletes. A 2000 study reported that young girls who did rhythmic gymnastics had a 10-fold greater risk of developing scoliosis. This elevated risk is likely due to three concurrent factors: an imbalance of weight on the spine, loose joints and a delayed onset of puberty. (Delayed menstruation is a common risk factor for all female competitive female athletes such as stress fractures and possibly scoliosis.)
Risk factors for the progression of curved scoliosis in affected children and adolescents
Once a mild curve is observed, the next step becomes more difficult, as it predicts whether or not the curve will progress to a more severe condition. Although as many as three in 100 teens have a condition that's serious enough to at least need observation, the likelihood of severity may be lower or above average depending on other factors.
• Being female or at a younger age at the onset of scoliosis increases your risk.
• The greater the bending angle, the greater the risk. At 20 degrees, only about 20% of the curves advance. However, young adults diagnosed with a 30 degree curve have a 60% risk of progression; With a 50 degree curve, the hazard is 90%.
• Girls who have low scoliosis and an unbalanced spine by more than an inch may be less likely to develop curves. Taller girls also appear to be at greater risk. Curvatures caused by congenital scoliosis (spine problems present at birth) may progress rapidly.
Risk factors for progression to scoliosis in adults
In rare cases, scoliosis may develop in adults who may have had unknown or untreated scoliosis in their youth. Osteoporosis or weak bones, a serious problem in many older adults, can cause mild curvatures to develop. (Osteoporosis itself is not a risk factor for the onset of new scoliosis.) However, in most cases, it is not known why adult curves progress.
How dangerous is scoliosis? Impact on the lungs and heart
The severity of scoliosis depends on the degree of curvature and whether it threatens vital organs, specifically the lungs and heart. Mild scoliosis effect (less than 20 degrees). Mild scoliosis is not serious and requires no treatment other than monitoring.
The effect of moderate scoliosis (between 25 and 70 degrees). It is still not clear if mild scoliosis causes major health problems. In one study, adults with mild scoliosis had normal lung function, although they had difficulty exercising.
The effect of severe scoliosis (more than 70 degrees). If the curvature exceeds 70 degrees, the severe twisting of the spine that occurs in skeletal scoliosis can cause the ribs to press on the lungs, restrict breathing and reduce oxygen levels. One study concluded that nearly two-thirds of patients with 90-degree curves and below had less than 80% of normal lung capacity. Abnormalities can also affect the heart and cause dangerous changes.
The effect of severe scoliosis (more than 100 degrees). Ultimately, if the curvature reaches more than 100 degrees, both the lungs and the heart can be injured. Patients with this level of risk are at risk of developing lung infections and pneumonia. Curves greater than 100 degrees increase the mortality rate, but this problem is very uncommon in America.
How is scoliosis diagnosed?
The severity of scoliosis and the need for treatment are determined by the extent of the curvature of the spine and the angle of rotation of the trunk (ATR). Both are measured in degrees. The two factors are usually related, so, for example, a person with a 20° spinal curve has a 5° ATR. This measurement used to be a standard for recommending treatment, although it is now known that up to 80% of 20° curves do not get worse. Scoliosis is diagnosed when the curve measures 11 degrees or more, but treatment is not usually required until the curve is 30 degrees and the ATR is 7 degrees.
physical examination
Forward bending test. A screening test often used in schools and in pediatric or primary care doctors' offices is called the forward bend test, in which the child bends forward with his arms hanging down, with feet together and knees straight. The curve of structural scoliosis is more pronounced when bending, and the examiner may notice an unbalanced rib cage, where one side is higher than the other, or other abnormalities. The forward bend test is not sensitive to deformities in the lower back, a very common site of scoliosis. Therefore, it misses about 15% of scoliosis cases, and many experts do not recommend this test as the only method for detecting scoliosis.
Other physical tests. The patient is usually asked to walk on the toes, then the heel, and then he is asked to jump up and down on one foot. These activities indicate leg strength and balance. The doctor will also check for tight tendons in the back of the leg, which is typical in adolescence, but may also indicate nerve root irritation or spondylolisthesis, a condition in which one vertebra slips forward over the other. The doctor will also check for nervous system dysfunction by testing reflexes, nerve sensation, and muscle function.
Recognize the curvature
Diagnosis
True is important, because poor judgment can lead to unnecessary X-rays and cumbersome treatments in children who are not at risk of progression. Unfortunately, although measurements of curves and rotation are useful, there is no test yet to determine whether or not a curve will advance. tilt (scoliometer). The clinometer (scoulometer) measures deformities of the trunk. The procedure is as follows:
The patient is asked to bend with outstretched arms and press the palms together, until a curve can be observed in the chest (upper back) area. The Scoliometer is placed on the back and is used to measure the apex (highest point) of the curve. Scoliometer results can indicate problems, and some experts believe it will be a useful tool for widespread screening. However, Scholetter's scales measure rib cage abnormalities in more than half of children who have been shown to have very little or no lateral curves. Scholetter's scales are not accurate enough to guide treatment, and if results show an abnormality, an X-ray should be performed.
Imaging tests
X-rays are currently the most cost-effective way to diagnose scoliosis. Experts hope that an accurate, non-invasive diagnostic technique can be developed that may eventually replace some of the X-rays currently used to monitor the progression of scoliosis. So far, some of these techniques appear to be fairly accurate for detecting scoliosis in the upper back (the thoracic region) but not scoliosis in the lower back (the woody region).
X ray. If the examination indicates scoliosis, the child may be sent to a specialist who takes an initial X-ray and monitors the child every few months with frequent X-rays. X-rays are necessary for the accurate diagnosis of scoliosis in several ways:
• X-rays reveal the degree and severity of scoliosis.
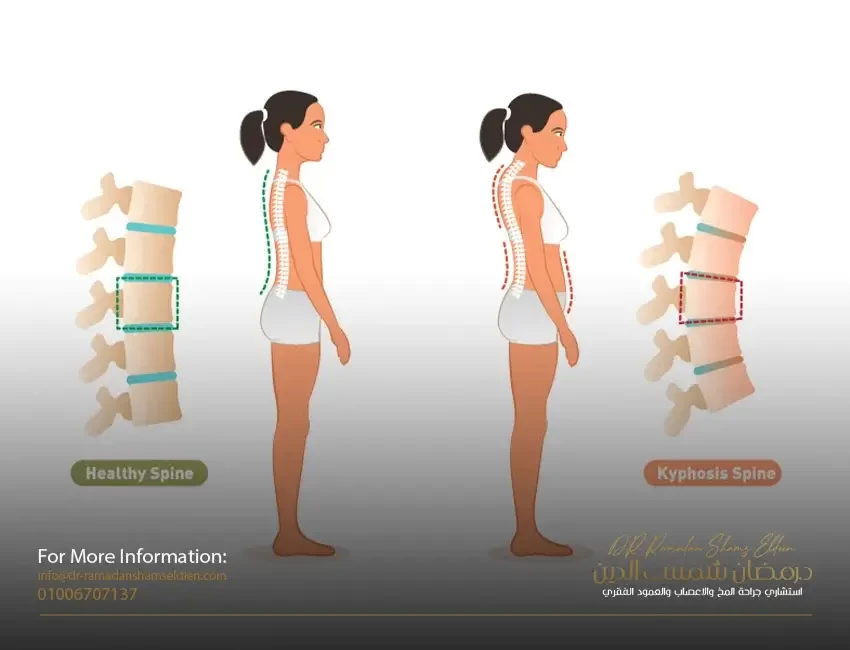
• An X-ray identifies any other abnormalities of the spine, including kyphosis (hunchback) and hyperlordosis (fluctuation).
• X-rays help the doctor determine whether the skeletal growth has reached maturity or not.
• X-rays of patients with curvature can help distinguish between structural and non-structural scoliosis.
Structural curves persist when a person bends, and non-structural curves tend to disappear. (It should be noted that sometimes muscle spasms or a growing spine can cause non-structural scoliosis, which shows a curve when bending.)
In children and adolescents with mild curvatures or in older adolescents with more severe curvatures, but whose growth has stopped or slowed, X-rays should be done every few months in order to detect the increased severity. Young adults with scoliosis should be sure to keep X-rays indefinitely in case back problems develop later in adulthood and need to be re-examined.
curve calculation
cup method. The degree of the curve is almost always calculated using a technique known as the Cobb method.
On an X-ray of the spine, the examiner draws two lines: one line that extends outward and upward from the upper vertebra edge of the curve. The second line extends outward and downward from the lower vertebrae. Then a vertical line is drawn between the two lines. The angle of intersection is measured to determine the degree of bending.
The Cobb method is limited because it cannot fully define the three dimensions of the spine. So they are not effective in determining spinal rotation or kyphosis. It also tends to overestimate the curve. Other diagnostic tools are needed to make a more accurate diagnosis.
A new technique that uses calculations based on geometric principles for the apex of the curve as well as the top and bottom of the curve to determine all dimensions of the curve may prove to be accurate.
Determine the end of growth
Even if the curve is calculated accurately, it is still difficult to predict whether or not scoliosis will progress. One way to predict whether or not the curvature will progress is to know when the child will stop growing. If a child has years to grow, the spine has more time to progress. If a child stops growing within a year, the progress should be very slight. (It should be noted, however, that some progression occurs in approximately 70% of the curves even after the spine has matured.)
Knowing a child's age is of course the first step in estimating the end of development. In addition, other methods have been developed to help predict the end of the growth phase.
One method is called the Risser's sign, which quantifies the amount of bone in the area at the top of the hip bone. A low score indicates that the skeleton still has significant growth; A high score means that the child has almost stopped growing and a small curve is unlikely to progress much further. The Rieser scale varies between genders and boys.
Scoliosis treatment has undergone significant changes over the past decade and a number of options are available.
treatment decision
The general rule for treating scoliosis is to monitor the condition if the curve is less than 20 degrees and consider treating curves greater than 25 degrees or those that progress by 10 degrees during monitoring. However, whether scoliosis is treated right away or just monitored is not an easy decision. The percentage of cases that will progress more than 5 degrees can be as low as 5% in certain cases and as high as 50% to 90% depending on severe curves or other predisposing factors:
• age. In general, the older the child, the less likely the curve will progress. Experts estimate that curves less than 19 degrees will progress by 10% in girls between the ages of 13 and 15 and 4% in children older than 15. (In some rare severe cases, the curvature may worsen even after treatment and the end of growth due to the pressure of body weight on the abnormal curvature.
• Gender. Girls are more likely to progress than boys.
• bending site
. Thoracic curves, those at the top of the spine, are more likely to develop from thoracolumbar curves or lumbar curves, those in the middle of the spine to the bottom.
• Intensity of bending. The higher the score, the more likely the lungs will be affected.
• The presence of other health conditions. Children in poor health may experience more stressful scoliosis treatments than other children. On the other hand, children with existing conditions that threaten lung and heart problems may need immediate and aggressive treatment.